
Trauma-Informed Kink: Being a Survivor Who’s Also Kinky | Second Banana
Both Things
Can Be True.
On being a trauma survivor who is also kinky, and how to navigate the territory honestly
The Thing Nobody Warned You Was Possible
You already know you’re kinky. You may also already know you’re a trauma survivor. What nobody prepared you for was how thoroughly these two things would turn out to occupy the same psychological and physical space — and how complicated it would feel to hold both of them at once.
BDSM practices involve, by design, the deliberate exploration of power, vulnerability, pain, restraint, and intense emotional exposure — which are also, not coincidentally, the exact territories where trauma lives. The overlap is not accidental. It is neurological. The same systems that were dysregulated by traumatic experience are the systems that kink engages most directly. Which is why kink can be, for trauma survivors, simultaneously one of the most healing and one of the most potentially destabilising things they do.
This piece is not a piece about whether trauma survivors should do kink. That’s not a question anyone else can answer. It is a piece about what the research says about the intersection of trauma and BDSM, what “trauma-informed” practice actually means in this context (for both the person with the trauma history and the people they play with), what to watch for, and how to navigate the territory with the honesty it deserves.
It is also a piece about why this community — Second Banana’s community specifically — is one of the better places to have this conversation.
What the Research Actually Says
The research on trauma survivors in BDSM communities is more nuanced and more interesting than either the “kink is inherently healing” position or the “kink re-traumatises survivors” position would suggest. Both positions exist in the literature and in the community. Both capture something real. Neither is the whole picture.
The Prevalence Overlap
Multiple studies examining BDSM community members have found elevated rates of trauma history — including sexual trauma — compared to general population samples. A 2015 study by Richters and colleagues found that BDSM practitioners were more likely than non-practitioners to report a history of sexual abuse, though the differences were smaller than popular assumption suggests. A 2013 study by Wismeijer and van Assen found the opposite on most psychological dimensions — BDSM practitioners showed better psychological outcomes than the general population — but that study didn’t specifically examine trauma histories.
What the overlapping research suggests is that the BDSM community contains a meaningful proportion of people with trauma histories, that this doesn’t appear to be driving worse psychological outcomes overall, and that the relationship between trauma history and kink engagement is not a simple one. People with trauma histories are drawn to BDSM for reasons that the research is only beginning to map, and the effects of that engagement vary enormously depending on how it’s approached.
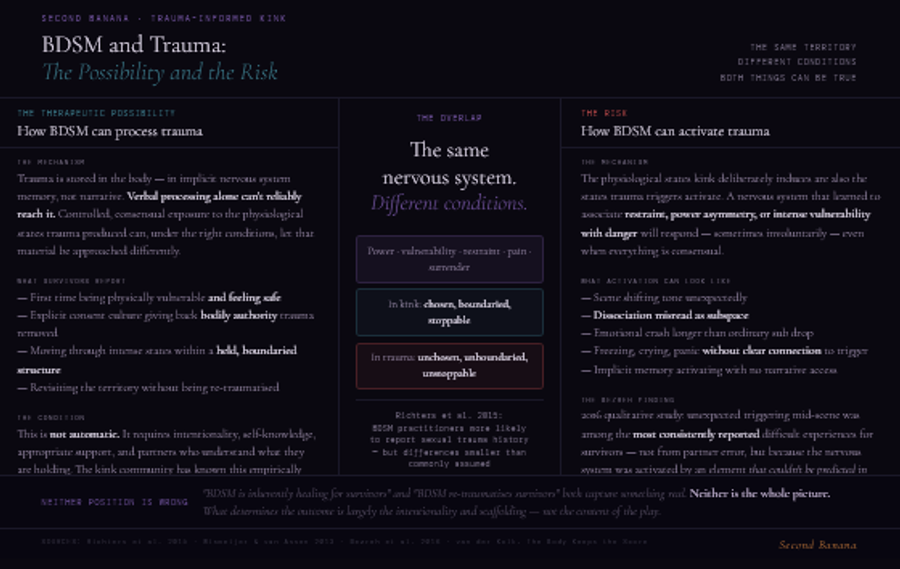
BDSM as Processing: The Therapeutic Possibility
A growing body of qualitative research — including work by social scientists Staci Newmahr and Margot Weiss examining BDSM communities, and the clinical observations of therapists including Raven Kaldera and Barbara Carrellas who work at the intersection of somatic therapy and kink — suggests that BDSM can function as a form of experiential processing for trauma survivors when engaged in deliberately and with adequate support.
The mechanism proposed is consistent with the broader somatic trauma research we covered in the shame and tantra pieces. Trauma is stored in the body — in the nervous system, in the implicit memory of the threat response, in the physical patterns of freeze, flight, and fight that were adaptive during the traumatic experience and that persist afterward. Verbal processing alone cannot reliably access this material. But controlled, consensual, boundaried exposure to the physiological states that trauma produced — intense arousal, vulnerability, the experience of being in the presence of someone with power over your body — can, under the right conditions, provide a context in which that material can be approached differently.
For some survivors, a BDSM scene provides the first context in which they have been physically vulnerable to another person and felt genuinely safe. For others, the explicit consent negotiation that good kink practice requires gives them an experience of having power over what happens to their body that trauma had previously removed. For others still, the specific experience of moving through intense physiological states — fear, pain, restraint, surrender — within a held, boundaried, consensual structure provides something that neither talk therapy nor daily life had offered: a way to revisit the territory of the trauma without being re-traumatised by it.
This is not automatic. It does not happen simply by virtue of doing kink. It requires intentionality, self-awareness, appropriate support, and partners who understand what they are holding. But it is real, and it is one of the things the kink community has known empirically for decades that clinical research is only now beginning to validate.
BDSM as Trigger: The Risk
The same research that documents the potential for BDSM to be healing is equally clear about the potential for it to be destabilising. The physiological states that kink deliberately induces — heightened arousal, physical restraint, pain, intense vulnerability, power asymmetry, the temporary loss of control — are also the states that trauma-related triggers activate. For a survivor whose nervous system has learned to associate these states with danger, kink engages the threat response directly and sometimes involuntarily.
This can look like: a scene that starts well and then suddenly shifts tone as a particular element unexpectedly activates a trauma response. Dissociation during play that can be misread by a partner as going deep into subspace. An emotional crash after a scene that is more intense and longer-lasting than ordinary sub drop. Physiological responses — freezing, involuntary crying, sudden panic — that arrive without clear cognitive connection to what triggered them. The activation of implicit memory that the person has no narrative access to but that the body is responding to viscerally.
A 2016 qualitative study by Bezreh and colleagues, examining trauma survivors’ experiences in BDSM contexts, found that unexpected triggering during scenes was one of the most consistently reported difficult experiences — not because the partners had done anything wrong, but because the survivor’s nervous system had been activated by an element that couldn’t be predicted in advance. The unpredictability is part of what makes this territory complex: you cannot always know in advance what will trigger you, which means you cannot always prevent it.
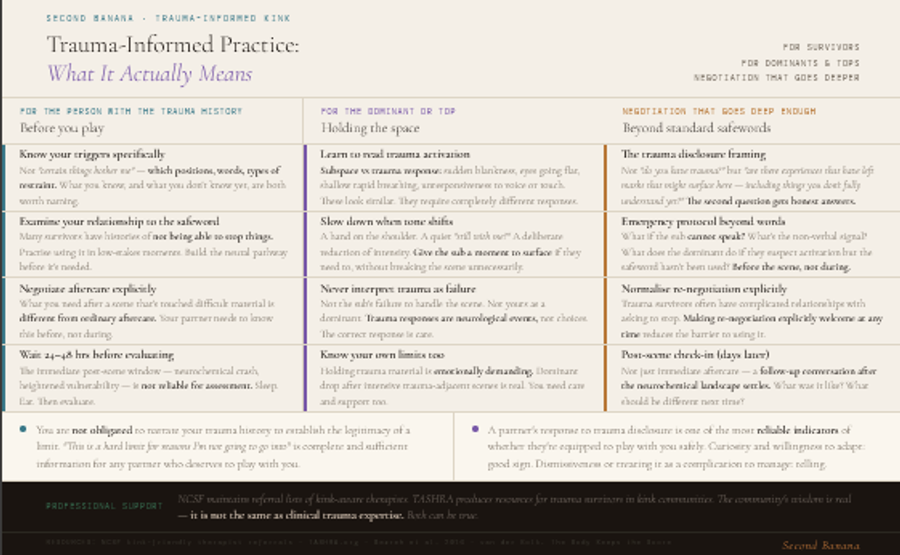
Trauma-Informed Practice: What It Actually Means
Trauma-informed practice, in medical and therapeutic contexts, refers to an approach that understands the widespread impact of trauma, recognises the signs and symptoms of trauma, integrates knowledge about trauma into practice, and actively avoids re-traumatisation. Translated into BDSM contexts, it means something specific and practical: practice that is conducted with awareness of the possibility of trauma history (in oneself or in a partner), that builds in structures to support safety and recovery, and that holds space for the unexpected without making it worse.
This is not the same as only doing “safe,” “mild,” or “restricted” kink. Trauma-informed practice can include intense and challenging scenes. What distinguishes it is the intentionality and the scaffolding, not the content.
For the Person With the Trauma History
The foundational question is honest self-knowledge: what do you know about your triggers, and what don’t you know yet? For many trauma survivors, the answer to the second question is substantially larger than the answer to the first. Trauma responses are not always neatly catalogued and consciously available. They emerge, sometimes, in response to stimuli that the conscious mind doesn’t connect to the original experience. Working with a trauma-aware therapist alongside kink engagement is not a requirement, but it is the most reliable way to develop the self-knowledge that trauma-informed kink requires.
Before playing, particularly with a new partner or in unfamiliar territory:
- Know your established triggers as specifically as possible, and communicate them. Not just certain things bother me but specific physical positions, certain words or tones, restraint above the waist, being ignored during aftercare — these are things I know to flag.
- Establish a safeword that you will actually use — and examine your relationship to using it. Many trauma survivors have histories of not being able to stop things. The safeword is not just a safety mechanism. It is the embodied experience of having permission to stop. Practising using it, including in low-stakes moments, builds the neural pathway to using it when it matters.
- Negotiate not just the scene but the aftercare explicitly. What you need after a scene that has gone into difficult territory is different from ordinary aftercare. Your partner needs to know this in advance.
- Give yourself permission to call a scene even when nothing “wrong” has happened. The body’s signals are valid even when the mind can’t explain them. You do not need a reason the other person would understand in order to stop.
- After a scene, particularly an intense one, give yourself significant time before evaluating whether it was a positive or negative experience. The immediate post-scene period, with its neurochemical crash and heightened vulnerability, is not a reliable time for assessment. Sleep, eat, drink water, give it 24-48 hours.
For the Dominant or Top
Holding space for a trauma survivor in kink is one of the most significant acts of trust and responsibility in the BDSM dynamic, and it requires specific skills and knowledge that go beyond the ordinary requirements of good dominant practice.
The most important thing a dominant or top can do when playing with someone who has disclosed a trauma history is develop genuine trauma literacy: understanding how trauma affects the nervous system, what trauma responses look like when they emerge during play, and how to distinguish between a sub going into subspace (which can look like dissociation) and a sub having an actual trauma response (which also looks like dissociation but is something entirely different that requires a different response).
- Learn to read the signs: sudden stillness or blankness that is qualitatively different from the sub’s previous presence in the scene, eyes going flat or distant, shallow rapid breathing that is not erotic, involuntary shaking or crying that doesn’t have the quality of the scene’s emotional tone, the sub becoming unresponsive to voice or touch. These can be signs of trauma activation rather than scene depth.
- Slow down and check in whenever the tone of a scene shifts unexpectedly. Not always an explicit verbal check-in — sometimes that can break the scene unnecessarily — but a hand on the shoulder, a quiet “hey, still with me?”, a deliberate reduction of intensity that gives the sub a moment to surface if they need to.
- Never interpret a trauma response as failure — either the sub’s failure to handle the scene or your failure as a dominant. Trauma responses are neurological events, not choices. The correct response is care, not disappointment.
- After a scene that has activated difficult material, extended and careful aftercare is not optional. The sub who has moved through trauma territory during a scene needs significantly more grounding, physical warmth, and reassurance than the ordinary post-scene protocol provides. Plan for this before the scene begins.
- Know your own limits. Holding trauma material is emotionally demanding. If you find yourself regularly holding significant trauma responses in your partners without your own support structure, you will burn out. Dominant drop, after intensive scenes with trauma-activated partners, is real. You need care too.
Negotiation That Goes Deep Enough
Standard kink negotiation — safewords, hard and soft limits, the basics of what is and isn’t on the table — is necessary but not sufficient when one or both parties have trauma histories. Trauma-informed negotiation goes deeper:
- The trauma disclosure conversation: not “do you have any trauma?” (too broad, too abstract) but “are there specific experiences that have left marks on your nervous system that might come up in this context? Things that might come up that you don’t fully understand yet?” The second framing invites more honest and more useful answers.
- Emergency protocol: beyond safewords, what happens if the sub cannot speak? What is the non-verbal signal? What does the dominant do if they suspect a trauma response and the sub hasn’t used the safeword? This conversation needs to happen before the scene, not during it.
- The re-negotiation norm: establishing explicitly that any part of the negotiated dynamic can be changed at any time, without requiring explanation or justification. Trauma survivors often have complicated relationships with asking for things to stop. Making re-negotiation explicitly normal and welcome reduces the barrier.
- Post-scene check-in protocol: agree in advance on a check-in in the days after an intense scene — not just immediate aftercare but a later conversation, once the neurochemical landscape has settled, about what the experience was like and what, if anything, should be different next time.
The Question of Whether to Disclose
Many trauma survivors in kink contexts grapple with whether, when, and how much to disclose their history to potential partners. This is a genuinely difficult question with no universal answer, and the difficulty is compounded by the same dynamics that make disclosure difficult in every intimate context: the risk of being treated differently, the risk of the information being used to manage rather than to understand you, the risk that the disclosure will change what the other person is willing to do with you.
A few things the research and the community’s accumulated wisdom support:
Disclosure before play is almost always worth it, even when it’s uncomfortable. The cost of a partner being unprepared for a trauma response mid-scene is higher than the cost of the pre-scene conversation. This doesn’t mean a full history. It means the specific information that is relevant to the specific thing you’re planning to do: “there are things that can come up for me in this kind of play, and here’s what that might look like and what I need if it does.”
You are not obligated to explain the origin of your triggers to anyone. You are not obligated to narrate your trauma history to establish the legitimacy of your limits. “This is a hard limit for reasons I’m not going to go into” is complete and sufficient information for any partner who deserves to be playing with you.
A partner’s response to a trauma disclosure is one of the most reliable indicators of whether they are equipped to play with you safely. A partner who responds with curiosity, care, and genuine willingness to adapt their approach is a good sign. A partner who becomes dismissive, uncomfortable, or who treats the disclosure as a complication to be managed rather than information to be integrated is telling you something important about what it will be like to be vulnerable with them.
CNC and Trauma: The Specific Conversation
Consensual non-consent — role-play that deliberately mimics non-consensual scenarios — deserves specific attention in the context of trauma, because it is the kink most likely to involve, engage, or activate trauma-related material, and the one where the intersection of kink and trauma is most acutely felt.
For many survivors of sexual trauma, CNC is either deeply off-limits or, counterintuitively, deeply compelling. The research on non-consent fantasy (covered in the erotic fiction piece) suggests that the appeal of CNC for survivors is not straightforwardly about re-enacting trauma — it is often about re-experiencing the physiological territory of the trauma in a context where everything is different: consent is present, power is negotiated, the person can stop at any point, and the outcome is known in advance to be okay.
This can be genuinely processing and healing. It can also be re-traumatising. The difference lies almost entirely in the quality of the preparation, the relationship between the parties, and the robustness of the scaffolding around the scene. CNC with a new partner, without substantial negotiation, without a robust emergency protocol, without significant aftercare planning, is a very different risk profile from CNC with a long-term trusted partner with whom the territory has been carefully mapped.
If CNC is something you’re drawn to and you have a trauma history: slower is always better, and the quality of the relationship and the preparation matters more than any other single factor.
Aftercare Is Not Optional. It Is Especially Not Optional Here.
We wrote an entire piece on aftercare. For trauma survivors engaging in kink, everything in that piece is true and then some. The neurochemical crash following an intense scene, the vulnerability window, the need for physical warmth and emotional presence — all of this is amplified when the scene has moved through trauma territory.
Specifically for trauma survivors: aftercare needs to include, or be followed by, a return to the felt sense of the present. Grounding techniques — naming five things you can see, feeling the texture of a blanket, holding something warm — are not supplementary niceties. They are the mechanism by which the nervous system is reminded that the intense experience is over, that the body is safe now, that the present is different from the past the trauma memory was visiting.
Solo aftercare matters enormously here. What you do in the hours and days after an intense scene that has stirred significant material — how much you eat and sleep, whether you give yourself gentleness, whether you are in contact with a trusted person who knows what you’ve been doing — is as important as the aftercare your partner provides immediately after the scene.
Professional Support: When the Work Needs More Than the Community Can Hold
The kink community can hold a great deal. It has genuine wisdom about trauma and BDSM, developed over decades of practical experience, and the community’s peer support structures are real and valuable. But there are things the community cannot hold, and it is important to be clear about where the limits are.
If you are regularly activating significant trauma responses during kink play; if you are finding that your kink engagement is increasing rather than decreasing your trauma symptoms over time; if you are using kink to avoid rather than engage with the processing your trauma requires; if your relationship to kink is feeling compulsive rather than chosen — these are signals that the work needs professional support alongside or instead of the community’s holding.
Therapists who are both trauma-informed and kink-aware exist, though they are not yet the majority. Organisations including NCSF (National Coalition for Sexual Freedom) maintain referral lists of kink-friendly therapists. The TASHRA (The Alternative Sexuality Health and Research Alliance) produces resources specifically for trauma survivors in the kink community. These are worth knowing about.
There is no shame in needing more than the community can provide. The kink community’s wisdom is real and substantial. It is not the same as clinical trauma expertise. Both can be true.
Second Banana and This Conversation
The anonymous posting model matters here in a way that is specific and significant. Disclosing a trauma history in a dating or connection context — particularly when that disclosure is specifically relevant to the kind of kink you’re interested in — requires a level of trust in the context that most platforms don’t earn before they ask for it. Second Banana’s model inverts this: you can be honest about what you carry and what you need before any specific person has the opportunity to respond to it badly.
The Second Banana tag system allows people to signal trauma-awareness as a requirement without having to explain why. Tags like “trauma-informed,” “pace matters,” “emotional safety first,” “experience with survivors,” “slowing down is not a problem” communicate clearly to the right person and serve as self-selection mechanisms for everyone else.
Both Things Can Be True
You can be a trauma survivor and a kinky person. These are not contradictory. They are not in tension in the way the culture sometimes implies — as though your trauma history should either put you off kink altogether or explain why you’re kinky in some reductive causal way. Most trauma survivors in kink communities didn’t become kinky because of their trauma. They were kinky before the trauma, or the trauma is entirely unrelated to their kink interests, or the relationship between the two is complicated and non-linear in ways that resist simple narrative.
What is true is that the overlap requires attention. The nervous system that was shaped by trauma is the same nervous system that engages with kink. That’s not a reason to avoid kink. It’s a reason to approach it with the honesty and intentionality and care that any complex territory deserves.
The kink community, at its best, has always known that what people bring to the dungeon is not separate from who they are outside it. That the vulnerability of a scene is real vulnerability. That the trust required for power exchange is real trust. That holding someone’s most difficult material, in a consensual and boundaried context, is one of the most profound things one person can do for another.
You don’t have to have it all figured out before you start. You have to be honest about where you are, find people who can meet you there, and build the scaffolding as you go. That’s always been the work.
Find the people who can hold what you carry. They’re here. 🍌


